1. Introduction: Assessing the Roadmap to 2025
The Health Sector Medium-Term Development Plan (HSMTDP 2022-2025) is Ghana’s primary strategic vehicle for achieving Universal Health Coverage (UHC) by 2030. Within the Ghanaian context, UHC is defined as ensuring that all people have timely access to high-quality health services irrespective of their ability to pay at the point of use. Between March and June 2024, the Ministry of Health (MoH) conducted a Mid-Term Review (MTR) to evaluate whether the sector’s current trajectory aligns with these 2030 aspirations.
The HSMTDP was designed to resolve five major health development issues:
- Inequitable distribution of human resources for health across regions.
- Inadequate health infrastructure, logistics, and medical equipment.
- Inequity in access to essential services and significant variability in service quality.
- Weak coordination and suboptimal harmonization between public and private providers.
- A weak referral and gatekeeper system.
——————————————————————————–
2. The Mid-Term Scorecard: Performance by the Numbers
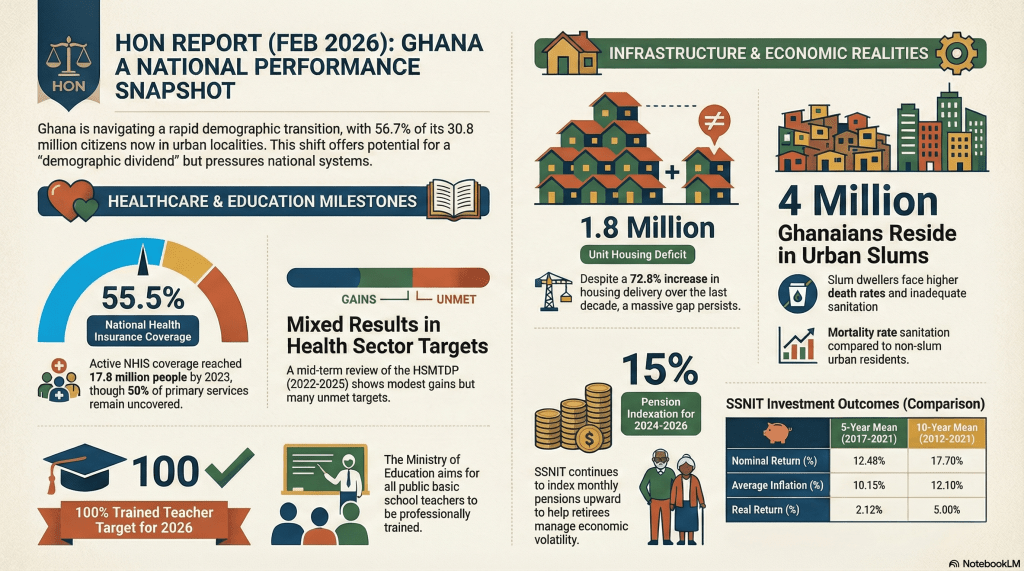
The MTR analyzed 124 quantitative indicators across four primary program areas. The findings reveal a landscape of “mixed results” where local resilience often masks systemic underperformance. A critical finding is the pervasive lack of data, particularly in human resource development, which undermines evidence-based policy making.
| Program Area | Total Indicators | Performance Summary (Targets Met vs. Progressed/Declined) |
|---|---|---|
| Management and Administration | 52 | 8 targets met; 11 progressed; 8 declined/below baseline; 25 lacked complete data. |
| Health Service Delivery | 51 | 15 targets met; 12 progressed; 4 fell below baseline; 20 lacked complete data/targets. |
| Human Resource Development | 13 | 0 targets met; 1 showed a production increase; 10 (77%) lacked data entirely. |
| Health Sector Regulation | 8 | 3 targets met; 1 fell below baseline; 4 lacked complete data. |
Key Insight: Only 20% (26 of 124) of the total indicators successfully met their mid-term 2023 targets. Most concerning is that 77% of Human Resource indicators had zero data available for the three-year review period, representing a critical failure in strategic monitoring.
——————————————————————————–
3. The “COVID-19 Legacy”: From Emergency Response to Systemic Resilience
The pandemic response served as a pivot point for Ghana’s health system, transitioning from a reactive emergency posture to a more resilient framework. These legacies must now be mainstreamed into routine operations to ensure they are not lost to history.
Hardware Legacies The sector inherited a permanent expansion of physical capacity:
- New Infectious Disease hospitals and dedicated isolation centers.
- Expanded critical care units and ICU facilities at the tertiary level.
- Enhanced national oxygen production capacity and modernized medical equipment.
Software Legacies The “software” of governance and readiness has seen a fundamental upgrade:
- Institutionalized Emergency Operation Centers (EOCs) and the conduct of regular emergency simulations.
- A strengthened network of public health laboratories and expanded Basic Life Saving (BLS) training.
- Integrated surveillance through the deployment of the SORMAS (Surveillance Outbreak Response Management & Analysis System).
——————————————————————————–
4. The Financing Gap: A State of “Operational Paralysis”
The MTR identifies a dangerous structural imbalance in health financing. While the government fulfills its obligations toward the workforce, funding for actual patient care has entered a state of operational paralysis.
- The Compensation Heavyweight: For Government of Ghana (GoG) funds, employee salaries and compensation account for above 95% of the total budget. The state essentially only pays for personnel, leaving service delivery entirely dependent on Internally Generated Funds (IGF) and donors.
- The Goods & Services Shortfall: Releases for operational funding have collapsed. In 2022, only 14% of the approved budget for GoG goods and services was released; by September 2023, this dropped to a negligible 5%.
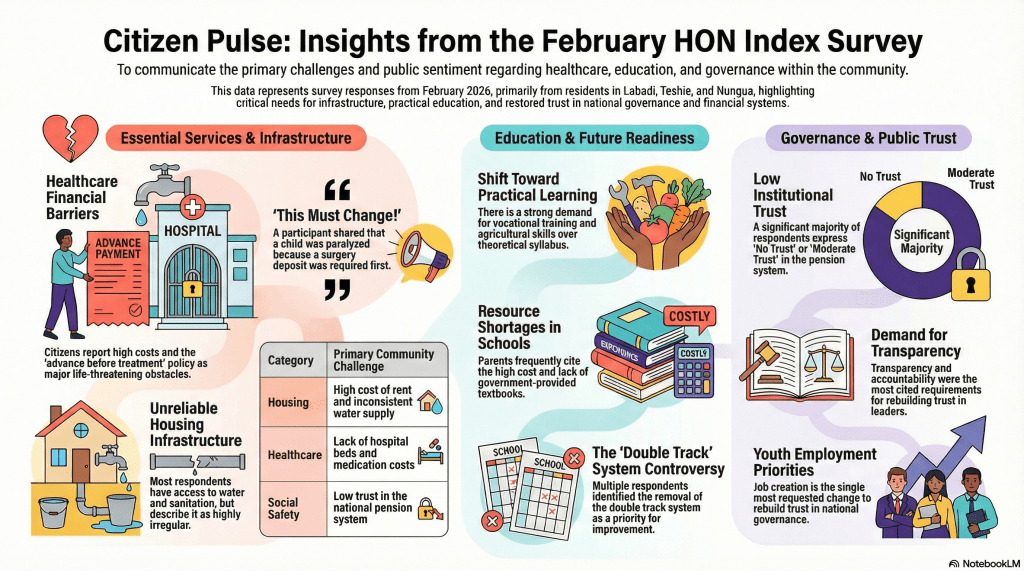
- Out-of-Pocket Realities: Despite the UHC goal to eliminate financial barriers, out-of-pocket (OOP) payments increased from 23.8% in 2020 to 25% in 2022, signaling a decline in financial risk protection.
- NHIS Barriers: While active coverage marginally increased to 55.5% in 2023, approximately 50% of primary care services remain uncovered by the insurance benefit package.
——————————————————————————–
5. Digitization and the Supply Chain Paradox
Ghana faces a stark paradox: high adoption of digital logistics tools alongside a persistent 49% stock-out rate for tracer medicines.
This supply chain crisis is largely driven by a debt cycle. National Health Insurance Scheme (NHIS) reimbursements are delayed by an average of 5–6 months. This delay prevents facilities from paying Regional Medical Stores, leading to facility indebtedness and subsequent commodity shortages.
The sector currently operates three primary digital tools—LHIMS, GhiLMIS, and SORMAS—but they exist as “data silos.” A lack of interoperability between these systems and DHIMS2 prevents a unified, real-time quantification of needs, which is essential for accurate forecasting.
——————————————————————————–
6. Health Workforce and Regulation: The Brain Drain Paradox
Ghana has successfully expanded the production of health professionals, yet this achievement has highlighted a systemic “Brain Drain Paradox.”
The Production vs. Employment Gap While the production of medical officers increased by 96.3% and nurses/midwives by 20.3% in 2022, the “budget crunch” means the government cannot afford to hire them. This results in the state training professionals for export, as many remain unemployed at home while existing staff migrate abroad in record numbers.
Rationalizing Regulation The Ministry now oversees over 30 semi-independent agencies. The MTR recommends a need to rationalize these agencies due to fragmentation and high administrative overhead. Regulatory capacity is struggling to keep pace with the expansion of the private sector and specialized care models like geriatric and palliative care.
——————————————————————————–
7. Strategic Pivot: Recommendations for the Final Stretch
To bridge the performance gap by 2025, the sector must shift from routine activities to catalytic policy interventions.
Governance and Operational Efficiency
- Agency Rationalization: Conduct cost-benefit analyses before creating new agencies to prevent further fragmentation.
- The Port Waiver Crisis: Streamline the acquisition of waivers to prevent life-saving medicines (HIV, TB, Malaria) from being held at the port for up to a year due to tax demands.
- GIFMIS Deployment: Accelerate the rollout of the Ghana Integrated Financial Management Information System to all subnational facilities to improve financial transparency.
Strategic Planning and NCDs
- Sin Taxes: Ringfence taxes on tobacco, alcohol, and sugar to fund the rising burden of Non-Communicable Diseases (NCDs), which now account for 45% of the disease burden.
- Networks of Practice (NoP): Pivot toward NoPs to coordinate public and private providers. A critical policy hurdle remains: the NHIA must transition from credentialing individual facilities to credentialing the entire network.
——————————————————————————–
8. Conclusion: Moving Toward a New Theory of Change
The primary finding of the Mid-Term Review is that the resilience of peripheral-level staff is the fragile foundation sustaining Ghana’s health system. These professionals solve local problems daily despite systemic financial bottlenecks and chronic stock-outs.
However, resilience is not a sustainable strategy for UHC. For the remainder of the HSMTDP period, the sector must abandon “business as usual” in favor of a robust Theory of Change. Success will require a decisive resource redirection—shifting focus from routine operations to the catalytic policy interventions and sustainable domestic financing models needed to make UHC a reality for all Ghanaians.

Leave a comment